Roger Clarke's Web-Site
© Xamax Consultancy Pty Ltd, 1995-2024

Infrastructure
& Privacy
Matilda
Roger Clarke's Web-Site© Xamax Consultancy Pty Ltd, 1995-2024 |
|
|||||
| HOME | eBusiness |
Information Infrastructure |
Dataveillance & Privacy |
Identity Matters | Other Topics | |
| What's New |
Waltzing Matilda | Advanced Site-Search | ||||
Draft Journal Article
Version of 20 February 2021
© Xamax Consultancy Pty Ltd, 2020-21
Available under an AEShareNet ![]() licence or a Creative
Commons
licence or a Creative
Commons  licence.
licence.
This document is at http://rogerclarke.com/EC/CVMJ.html
The COVID-19 pandemic has presented governments with challenges not only in relation to bio-medical understanding, medical treatment and health facility operations, but also the management of public health, public behaviour and the economy. In the area of public health management, discrete event simulation (DES) modelling is capable of providing considerable assistance to decision-makers. In April 2020, on the basis of publicly available information about the virus and its impacts, an analysis was undertaken of the needs of public health policy-makers, and a 16-state / 40-flow model was postulated. The model was revisited in December 2020, and experiences around the world applied in order to evaluate the model's apparent usefulness. This resulted in improved appreciation of its applicability and limitations, and a revised model. That model is capable of assisting teams of policy-makers to ensure commonality of understanding of environmental factors and to assess the likely impacts of alternative interventions.
There has long been contention between broad and narrow interpretations of the scope of the information system discipline. A broad view has as its focal point information and its handling by any entity for any purpose, whereas narrower conceptions restrict the scope to information-handling by organisations, and even to its handling for the purposes of the organisation alone. From the broad to the narrow end of the spectrum, the range of stakeholders whose interests are reflected in IS research reduces from all to just one.
This article is a contribution towards the broad end of that spectrum. It is concerned with information handling for decision support in relation to a particular, high-profile public policy matter. The COVID-19 pandemic gave rise to a wide range of needs among policy-makers. The opportunity therefore exists for the conception, design and conduct of research oriented towards those needs. This article has as its focus one particular aspect among the many: the needs of organisations and individuals responsible for public health management, a challenge confronting governments in every jurisdiction in the world.
The notion of 'public policy' is, glibly, about "who gets what, when, how" (Knill & Tosun 2020, p.1). It is concerned with "matters of national or regional significance". It "involves enunciating objectives and principles; formulating steps to achieve them through legal and other regulatory measures; allocating resources; and conceiving, articulating, and implementing programs of action. Objectives are not just economic but social and environmental. Fulfilling policy objectives depends on cooperation among disparate organizations that often come from all sectors (public, private and voluntary)" (Niederman et al. 2017, p.5). It is also intrinsically political, in the sense that it involves the exercise of power relationships among those parties that have an interest in determining or at least influencing outcomes.
Provided that a broad interpretation of IS adopted, research whose purpose is to assist public policy decision-making has legitimacy within the discipline. However, despite early work on the role of information systems in policy making (e.g. Kling 1978), its treatment is sparse, and some movements have been subverted from their original intention.
For example, the field variously referred to as 'Green IS' and 'Sustainability' was conceived as having its focus on sustainability across the economy, through the use of information systems to achieve environmental objectives (Watson 2008, Dedrick 2010). The view of vom Brocke et al. (2013) was that "we need to start solving significant social problems, and we believe Green IS is the best candidate that we have" (p.510). This intention remains, as evidenced in, for example, a Call for Papers for AMCIS'21, which declares that "Sustainable management aspires towards balancing and integrating social, economic and environmental dimensions". On the other hand, a considerable proportion of the published research in the area addresses corporate concerns about costs and public image.
A check was performed of the occurrence of {"public policy", disaster, pandemic, epidemic} in title, abstract and keywords of the Basket of 8 journals, and two relevant specialist journals, Information Technology & People (IT&P), and Decision Support Systems (DSS). This found 38 articles for "public policy" and 15 for "disaster", in a combined corpus of over 9,000 in the Basket of 8 (4 and 2 per mille). IT&P also offered only a small number, although twice the proportion in the Basket of 8. DSS offered far fewer for "public policy", but considerably more for "disaster". Given the topic of the present paper, it is noteworthy that the terms "pandemic" and "epidemic" scored respectively only 6 in Basket of 8 journals, 0 in IT&P, and 6 in DSS (overall, 1 per mille).
This of course understates the volume of research that is conducted, and conference papers and journal articles that are published, that are relevant to public policy. However, the majority are in sub-fields that address specific application areas, such as community information systems and Information and Communications Technology for Development (ICT4D) - areas that attract relatively small numbers of scholars, generate few papers in the most prestigious venues, and seldom achieve large citation-counts.
Another analysis that highlights the paucity of research in public policy areas considers the stakeholder perspective adopted by researchers. Across a variety of venues, including but extending beyond the Basket of 8, around 90% of published works have as their focus the interests of the information systems sponsor, with other stakeholders' interests considered only as constraints on the attainment of the sponsor's objectives (Clarke et al. 2020a, 2020b).
The present article seeks to make a contribution to public policy in relation to the management of public health in the context of a pandemic, and to reflect a wide range of stakeholder interests. From time to time, viral epidemics within individual countries threaten the health and lives of the country's inhabitants, and may wreak havoc on social and economic activities. Once the threat has passed, recovery may be quite brisk, provided that the country is sufficiently economically open. Global pandemics, on the other hand, harbour the potential for health impacts over large regions and potentially the whole world, and may have longer-term impacts on economic wellbeing because all countries' economies have been hampered and hence drivers of recovery are in short supply.
A century after 'The Maybe-Spanish Flu' at the end of World War I, commencing about the beginning of 2020, the world was subjected to 'The Maybe-Chinese Coronavirus'. Naturally, ways were sought in which information technology (IT) could play a constructive role in the public response to the pandemic. Foreground needs existed in the areas of prevention and treatment of the conditions that afflict patients. The particular need that is the focus of the present paper was for assistance in public health interventions that are intended to slow the spread of the virus, to protect particularly vulnerable sub-populations, and ensure capacity to treat sufferers, and ultimately to defeat the virus, while sustaining public confidence and achieving sufficiently high levels of compliance.
Emergency funding was provided to enable experiments with medical tools (e.g. for infection-testing, antibody-testing, symptom treatments, discovery of the modes of transmission, spread-containment mechanisms and vaccination) and with computing tools (e.g. for contact-detection, proximity-monitoring, contact-tracing, data management and decision support). As is to be expected of urgent, rapidly-performed experiments with available tools and the brisk conception and development of new tools, a great many projects were ineffective and short-lived. A few, however, delivered very considerable benefits to individuals, societies and economies.
IT's contributions to decision-making about public health policy during this period have, on the other hand, been at best mediocre, despite the urgency of the need. Data gathering, reporting and graphical presentation are helpful, but far from adequate assistance to decision-makers, and in any case data collection and analysis have been haphazard and often ill-informed. To constitute information, and to enable the people responsible for public health management to make decisions, data must have context. That context may be provided by each individual policy-maker's own mental model. However, major programmes of this nature involve many stakeholders with diverse perspectives. The context is therefore multi-dimensional, it features competition among values, and the conception of the problem-space needs to be shared rather than personal.
The most powerful form of context is provided by models that are shared, that impose some degree of formality on the problem-space, that are sufficiently graphic that all stakeholders can relate to them, and that have an associated terminology that is reasonably common among the stakeholders. Given such a model, it becomes much easier to identify data that would be valuable input to deliberations, to generate and evaluate alternative courses of action, and to assess both the potential and the actual impacts of interventions.
The focus of this article is on a particular form of modelling tool, commonly referred to as 'discrete-event simulation' (DES). DES modelling enables expression of a model that represents a set of COVID-19 states that individuals may pass through, the conditions that determine the paths they follow, and key characteristics of both the states and the transitions. Research was conducted whose purpose was to postulate a model, apply it, assess its efficacy and improve it, in order to support mind-experiments and conversations about the real world into which public policy-makers were injecting successive interventions and refinements of interventions.
A DES model is a socio-technical artefact as that term is used in design science (Niederman & March 2012, Gregor & Hevner 2013, p.337). The process described by Peffers' Design Science Research Methodology (DSRM) commences with problem identification and definition of objectives, and is followed by design and development (Peffers et al. 2007). Peffers et al. distinguish two related phases towards the end of the design research approach. 'Demonstration' of the use of the artifact solves one or more instances of the problem (e.g. by means of experimentation, simulation or case study), whereas 'evaluation' involves more formal observation and measurement of the new artefact's effectiveness in addressing stated objectives. This research included Peffers phases of Problem Definition, Objectives Definition, Design and Expression, and a Demonstration step.
An alternative proposition, however, is that of Action Design Research (ADR), which argues that "the research process [contains] the inseparable and inherently interwoven activities of building the IT artifact, intervening in the organization, and evaluating it concurrently" (Sein et al. 2011, p.37). Similarly, both Soft Design Science Methodology (SDSM - Baskerville et al. 2009) and Participatory Action Design Research (PADR - Bilandzic and Venable 2011) regard evaluation as necessarily being, like quality assurance, an embedded and cyclical activity rather than just a back-end task. The process performed in this project expressly involved rounds of assessment of the emergent model on the basis of a great deal of information reported in a wide variety of venues, and has accordingly reflected this aspect of the ADR, SDSM and PADR approaches, as well as reflecting the importance of a back-end evaluation phase.
The paper commences by briefly summarising key features of the COVID-19 pandemic during the period March to December 2020. This is followed by a brief scan of relevant applications of IT that were prominent during 2020. An outline is then provided of the scope for modelling to assist, at various levels of investigation and decision-making. It is argued that discrete-event simulation modelling has a good fit to the needs of public health management. A model is presented that was devised in April 2020 on the basis of then-available information about the pandemic and government responses to it. Developments in the field during the following eight months are identified, and their implications for that model are investigated. It is concluded that such a model can provide an effective contribution by IT to the decision processes of public health policy-makers.
The new virus first came to public notice in the form of an epidemic in the Chinese city of Wuhan beginning in December 2019. Unsurprisingly, it took some time to be recognised and then accepted as a serious threat to public health. On 11 March 2020, based on rapid growth in detected case-numbers in northern Italy, Iran and South Korea, the World Health Organisation (WHO) declared a pandemic. By the end of March 2020, it had exploded in the USA, Spain, Germany and France, with rapid spread emergent in many other countries.
In most countries, there was an early peak of infections lasting 2-4 months with deaths following after a 1-3 week lag, then a lull, then 6-8 months later a 'second wave' in many cases worse than the first (Econ 2020). By the end of 2020, substantial second waves were infecting very large numbers of people and killing large numbers, with the cumulative (known) case-count worldwide past 80m and the death-count approaching 2m. On these measures, only two pandemics of the last century have been worse: the 'Spanish Flu' of 1918-20, and HIV/AIDS since 1980.
The cause was identified as a form of coronavirus, spread primarily by an infected person coughing or sneezing, or perhaps even speaking or breathing out, contaminated droplets (over a range of perhaps 1m), or possibly aerosols or droplet nuclei (very small droplets, over a range of perhaps 3-4m), or by direct contact with another person, or by contaminating 'fomites', i.e. objects and surfaces in the infectee's immediate environment (WHO 2020b).
Susceptibility appeared to be quite low under 10 years of age, increasing with age, and very high for those over 70. Impacts on individuals ranged from short-term, unpleasant but variable experiences, to very serious lung malfunction and death from that or consequential causes. Over time, it became apparent that there are small but significant numbers of people who suffer impacts for an extended period after the initial (predominantly pulmonary) impact of the virus (SWPRS 2020). However, most infectees are asymptomatic, decreasing the likelihood of detection and hence increasing the likelihood of spread.
A person with the virus may be infectious from 1-3 days before symptom onset, then for a further 1-2 weeks for asymptomatic persons, up to 3 weeks in mild to moderate cases, but much longer in severe cases (WHO 2020c). There were no known treatments for the virus itself. The proportion of hospitalised patients needing admission to Intensive Care Units (ICUs) ranged from 5% to 15%. In some regions, ICU capacity proved inadequate.
Mortality was very heavily skewed towards people over 70, with the likelihood of death much higher for those with bronchial and some other relevant or otherwise debilitating conditions. Employees in hospitals and aged care homes were at risk of high viral load, and high-quality hygiene and personal protective equipment (PPE) were essential. Despite precautions, many health care workers succumbed. They constituted about 1% of the USA's over 300,000 deaths during 2020 (Gn 2020b).
The focus of public health actions was on the prevention of spread, most urgently among those at greatest risk. The public health imperative is constrained by the limitations of enforcement powers and resources, and by conflict with freedoms of action and movement, and with economic management. In some jurisdictions, those challenges were exacerbated by a lack of political will. Countries adopted varying approaches to public health management, with highly varying senses of urgency, varying levels of compliance by the public, and highly varying case-counts, fatality-counts and fatality-rates (WOM 2020).
A variety of approaches were apparent to the application of IS and IT in support of the worldwide effort to combat the pandemic. An early review is in Budd et al. (2020). This section briefly reviews several categories of initiative.
Considerable hope was vested in support for contact-detection and -tracing by means of apps that used Bluetooth Relative Signal Strength Indicator (RSSI) readings, as detected by mobile-phones and tablets, as a proxy for proximity between the individuals they belonged to (Ahmed et al. 2020). Some of these experiments derived from marketing applications of RSSI, and others may have been revivals of predecessor experiments in relation to flu transmission, using mobile phones for proximity-detection by means of Bluetooth and GPS-based location-data (Yoneki 2011).
Projects were implemented throughout the world, with great fanfare and high hopes. They reflected several different models, characterised by (Riemer et al. 2020) as Surveillance Tracing (adopted in China, Israel and South Korea), Centralised Proximity Tracing (e.g. in Singapore and Australia) and Decentralised Proximity Tracing (notably the Apple-Google Privacy-Preserving Contact Tracing approach - AG 2020). All such apps faced enormous practical challenges, variously of a technical nature (Clarke 2020a, Mussared & Teague 2020), a social nature (Rowe et al. 2020), and a collective action governance nature (Riemer et al. 2020). As a result, they have contributed very little to contact-tracing (de la Garza 2020). The technical difficulties may well be intractable; however, for a survey-based assessment of the app specifications that appear to be salient for mass acceptance, see Trang et al (2020).
Another use of handheld apps emerged as lockdowns were eased, and visits to entertainment venues were again permitted. These involved handhelds being used to photograph a QR-Code and submit pre-recorded personal details into centrally-stored venue-attendance registers (Nguyen 2020). Such technically simple schemes could be capable of reasonably high degrees of effectiveness. They gave rise to concern, however, because the storage and access mechanisms were opaque (Greenleaf 2020). Some governments issued apps, and even mandated their use, but that also raised concerns about the data's storage, longevity and availability.
As the possibility of mass vaccination emerged, more record-keeping systems needed to be adapted, and another family of apps emerged that was claimed to enable individuals to provide evidence, in the form of 'vaccination passports', e.g. to airlines prior to boarding (ALI 2021). Doubts rapidly emerged about the effectiveness, reliability and robustness of such schemes, the security of the associated data, and the manageability of their negative privacy impacts (Loughran 2021).
A conventional form of IS support is the facilitation and management of data collection, data processing and database maintenance. Several categories of data were involved. Much of it related to individual cases, including information about the individual, the source and nature of the infection, treatments, pathways, outcomes, and for large number of people, the cause(s) of death. Data was also needed about people who had been in proximity to infectees, about the availability and disposition of treatment facilities, and by the end of 2020, vaccinations. Systems were upgraded, newly developed or re-purposed to address the needs. They evidenced diversity, of data-items, of data definitions and of business processing specifications, resulting in limitations on inter-operability and hence on the processing and analysis of merged data collections.
The urgency resulted in the short-changing of problem analysis, process and data-model design, and system configuration. In some cases, privacy sensitivity was built into designs, but most appeared to have been flung together with a tight focus on the intended functionality, and little awareness of the contexts of use. As a result, many such schemes involved centralised databases and the absence of infrastructural protections against second-party function creep and third-party access. A further factor in public distrust of these schemes was the strong impression they conveyed that such privacy safeguards as the law appeared to provide were able to be quickly and easily jettisoned, using urgency and/or public security justifications. In some countries, the involvement of national security agencies in the process exacerbated public suspicions. Concerns arose about the routinisation and embedment of population surveillance (Greenleaf & Kemp 2020, Clarke 2020b).
A further approach to the use of IS and IT was the rapid emergence of dynamic and entertaining graphical presentations of such data as was available. An excellent example is a "racing bar chart" of "Case number running totals by country", at Flourish (2020). The quality of the display hides the fact that the value of the information is very low. 'Case Numbers' is not a meaningful or reliable metric, because it is actually only 'Detected Case Numbers', and it is very challenging to devise a reliable estimator for 'Undetected Cases' and hence for 'Total Infectees'. Further, the 'Detected Cases' counts are generally not comparable, because the testing regimes, methods and population-samples have varied enormously over both space and time, even within individual jurisdictions, let alone across countries. These variations appear likely to be a significant factor in the enormous inter-country differences in the proportions of 'cases' who were admitted to hospital, who were admitted to intensive care units (ICUs), who survived, and who died.
Another misleading metric, which was championed for a time during April 2020 as "the one COVID-19 number to watch", was "the growth factor", as measured by the number of new cases reported on any one day in relation to those on the previous day (Elvery et al. 2020). Unless the sample tested is both purpose-selected and consistent, it is completely unclear what the positive-test ratio indicates. Case recognition is dependent on highly varied testing regimes, methods and population-samples. There is even debate about what constitutes 'a case of COVID-19' (Heneghan & Jefferson 2020). Yet 'case-count mania' continued as late as December 2020, with more useful information often marginalised.
Another inadequacy was the reporting of metrics on a per-country basis, despite the enormous disparity in countries' populations. To make comparisons, a normalised basis was needed, such as counts per million, or per 100,000. In addition, given the disparity of impact, there was a need to distinguish among sub-populations to reflect the degree of risk of infection and the probabilities of serious health consequences.
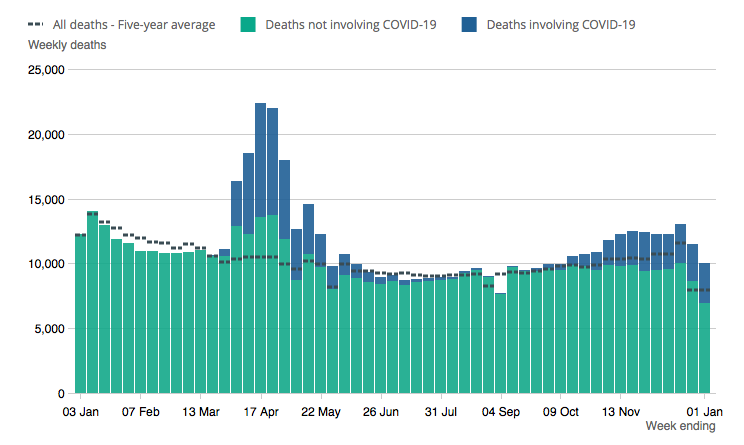
An example of data that provides both a sense of proportion and the scope to undertake more careful analyses is numbers and rates of 'excess deaths', also called 'excess mortality'. This is the number of deaths above the number expected on the basis of prior data, expressed as a proportion of the expected death-count (Econ 2020b). One study found that, for 15 weeks from mid-February 2020, it ranged across 21 countries from slightly negative to +100 deaths per million. This reflected additional deaths arising directly from COVID, or indirectly (e.g. failure to go to hospital after a heart-attack because of a fear of catching COVID), but also fewer deaths as a result of COVID (e.g. due to reduced time on the road) (Kontis et al. 2020). Another study of the timeline through 2020 has shown considerable variability across countries (Giattino et al. (2020).
An exemplary use of graphics to convey relevant information is in Figure 1 (ONS 2021). This clearly shows both the 'excess deaths' from COVID during the two waves, and the 'reduced deaths' from causes other than COVID.
Excess mortality is a metric that can be of value in understanding the relevant real-world system. Further categories of potentially valuable data are identified in Table 1. Most of this data was, and is, difficult even to capture, let alone to capture reliably and accurately. On the other hand, an assessment of the potential value of such data represents useful input to the question of what data should be prioritised for reliable collection.
Death counts, distinguished into sub-sets, depending on
whether COVID-19 was:
• the cause of death
• a significant factor in the death
(e.g. compounding prior conditions)
• otherwise known to be present at death
• assumed present at death • not known to be present at death | Death rates related to:
• normal death rates at the time-of-year
(in order to estimate 'excess deaths')
• population-size (to enable comparisons between geographical areas and jurisdictions) |
Results of tests for presence of the virus, using random
samples:
• of the whole population • of specific at-risk populations | Proportions tested for presence of the virus:
• of the whole population • of specific at-risk populations |
Hospital:
• admissions
• successful and unsuccessful discharges
ICU:
• admissions • successful and unsuccessful discharges | Results of tests for the presence of virus-specific antibodies
(as a proxy for prior exposure, for prior infectiousness, and/or for immunity),
using random samples:
• of the whole population • of specific at-risk populations |
For targeted action to halt spread, at-risk segments need to be postulated, and sampling conducted within those segments. Segments might be defined by geographical area, by age, by gender, by predisposing, chronic or debilitating condition (particularly bronchial and cardiac), by type of accommodation (with particular attention paid to communal and other close living, such as dormitories, prisons and aged care homes), and by intensive-exposure circumstances such as hospitals.
On the one hand, there has been evidence of poor-quality data and poor-quality analysis, particularly where the data-gathering and data analysis was ad hoc or opportunistic. On the other hand, some of these activities have delivered value. The remainder of this paper investigates the question as to whether the seeming absence of an 'enterprise model' of the undertaking and of 'data models' or 'information architecture' to support such a model, have hampered the potential contribution of IS and IT, and hence whether return on investment in IT can be improved by applying insights from modelling theory and practice.
A model is a simplified representation of a real-world system, which reflects interdependence among the relevant entities, structures and processes. Real-world socio-economic systems are open, complex and highly inter-connected. Simplification necessarily involves limiting the scope of the model, by placing the focus on one sub-system or two or more closely-related sub-systems, at one particular level of abstraction, and by excluding some factors and using proxies for others (Gault et al. 1987). A model therefore cannot replicate the real-world system (von Bertalanffy 1968). However, if key factors are appropriately reflected, experimentation with a model can deliver insights. At the very least, experimentation can suggest what data might be the most valuable to collect. In addition, participation in the modelling process may enhance observers' understanding of the world, and assist in making decisions about actions to take.
Early applications of computing to administrative data, from 1952, were characterised as data processing systems (DP). Applications that extracted and reported data of assistance in operational activities, from c.1970, were referred to as management information systems (MIS). Then decision support systems (DSS) used available data from operational support systems, combined with hypothetical or synthetic data, to enable 'what-if' investigations, and hence support strategic rather than tactical activities. The implicit models that had lain hidden beneath DP and MIS were no longer adequate. Strategic thinking demands greater clarity about models of the relevant current and possible future realities: " ... DSS ... became characterized as interactive computer based systems, which help decision makers utilize data and models to solve unstructured problems" (Sprague 1980, p.1).
During the first quarter of 2020, it became clear that COVID-19 had a high infection-rate and was life-threatening for some categories of people. As the epidemic in Wuhan developed into a pandemic, models were applied by a variety of people in a variety of contexts, in an endeavour to support various decision-makers. The remainder of this section briefly reviews the use of modelling in relation to the COVID-19 pandemic, based on public sources. The conclusion is reached that most models that have been publicly visible have been too narrow in their focus to satisfactorily support the needs of public health management. This suggests that the opportunity exists for more substantial contributions by IS and IT in those areas.
The most common form of model that was referred to during the pandemic was epidemiological models, most commonly of the SEIR(D) family. Many documents that report on applications of that model provide no operational definitions for the key concepts. They use the terms as though they were so well-understood, and so consistently applied, that declaration of their meaning, and discussion of those meanings' appropriateness to purpose, were redundant.
The underlying SIR model appears to have arisen from Kermack & McKendrick (1927). The primary reference for the SEIR model appears to be Aron & Schwartz (1984). This treats the population as comprising four groups:
Occasionally the following is added, particularly in the case of Ebola (Weitz & Dushoff 2015):
One of the few works to appear in the IS literature during 2020 applied a SIRD model (Pietz et al. 2020). Further variants that are apparent include:
Leakage from each state is sometimes acknowledged, in the form of a proportion of the count who die while within that state. However, there is commonly little or no discussion of the meanings of the terms used in the models, or of their relationship to the real world. In particular, the definitions of Q and J in these models may not accord with those used in the field.
Relevantly to the purpose of the present article, Silva et al. (2020) endeavours to use the SEIR model to investigate "scenarios of social distancing interventions ... with varying epidemiological and economic effects: (1) do nothing, (2) lockdown, (3) conditional lockdown, (4) vertical isolation, (5) partial isolation, (6) use of face masks, and (7) use of face masks together with 50% of adhesion to social isolation" (p.1). In Nikulin et al. (2020) the extended SEQIJR frame in Brauer (2008) was applied to model "the mitigation of the [COVID-19] virus via quarantine/isolation measures" (p.18). The authors also trialled a HIRD model (Healthy, Infected, Recovered, Dead) (pp.44-46). Another team applied established 'clinical pathway models' to assess the capacity of the Australian health system to cope with the COVID-19 pandemic. They concluded that isolation and quarantine alone would be insufficient (Moss et al. 2020).
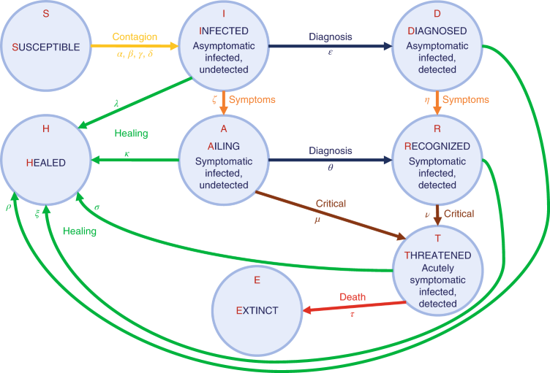
In Giordano et al. (2020), a new form of model was proposed with "eight stages of infection: susceptible (S), infected (I), diagnosed (D), ailing (A), recognized (R), threatened (T), healed (H) and extinct (E), collectively termed SIDARTHE" (p.1). This drops Infective and substitutes five categories of Infected (A/Symptomatic, Un/Diagnosed, plus Acutely Ill). See Figure 2.
Generally, models in the SEIR(D) family lack details needed for public health management purposes. There also appear to be material differences among, on the one hand, the meanings of the concepts as they are used in the various models, and, on the other, the definitions of the empirical data whereby associations between model results and real-world behaviours are asserted.
In addition to the A/Symptomatic and Un/Diagnosed states, hospitalisation and ICU are very important to public health management. There is also a need to be able to reflect new instances arriving into the population, and perhaps directly into intermediate states (e.g. ailing air- and sea-crew into hospital and even directly into ICU). The assumptions that people who have recovered are both no longer infective and no longer susceptible may also need to be tested.
In any case, it appears that all such models may only be able to represent intermediate states such as quarantine, isolation, hospitalisation and ICU-admission by means of variations in parameters, rather than by explicit representation. This reflects the orientation of this form of modelling towards mathematical approaches to decision-making. There are doubts about the usefulness of such approaches in environments of complexity, uncertainty, value conflicts, changing contexts and adaptive policies. "For a long time, differential equation ... models of disease states known as SIR models ... have been the primary modelling technique for understanding the spread of infectious disease. These models have [provided] information about tipping points and inform[ed] policy decisions. But ... these models are not adequate for modelling the human behavioural aspects that are important in disease transmission and epidemic dynamics" (Siebers et al. 2010, p.206).
In Schipper (2020), it is argued that modelling failed us during the COVID pandemic, because "the current epidemic model is medical, and narrowly so", "the current model recognizes the existence of cultural and other 'external' factors, but does not allow them to influence the model's projections or guidance", and "the model does not consider, let alone factor in even the direct health consequences of major economic disruption" (pp. 7-9). The author called for "a next generation epidemic model that goes beyond our current model ... to include:
This paper adopts the position that appropriate support by IS and IT for public-policy decision-makers in dynamic contexts like a pandemic depends on the application of appropriate modelling techniques. The techniques need to be instrumentalist, with a social-engineering orientation. Such models depend on careful definition of the system scope, and the level of abstraction at which the system is being observed. Key requirements of public health management are the establishment and progressive adaptation of a model that clearly distinguishes start-point(s), states, transitions, and end-point(s), and that identifies key attributes of each individual passing through the model (e.g. age-range and relevant-prior-conditions), and supports experimentation with different distributions of those variables.
The following section postulates such a model. The adequacy of the model is then tested against the phenomena and interpretations of them reported during the following 8 months of 2020, and adaptations are proposed in an endeavour to improve the model's capacity to assist policy-makers.
This section first discusses particular needs that arose during the COVID-19 pandemic in 2020, then outlines the relevant form of modelling, and finally describes an application of it that is argued to be of benefit to policy-makers.
Modelling at the bio-medical and medical levels ran in overdrive through 2020, but in specialist areas with limited public visibility. Economic models were also in use. The most apparent forms, however, were epidemiological models. These are well-established. They focus on parts of the health facility management and public health management levels, but they reflect only a limited sub-set of the factors that must be considered even in hospitals, let alone in workplaces, out on the streets, in transport, and in entertainment venues. In addition, they are 'socio-medical scientific' models that are designed to deliver understanding, rather than 'socio-medical engineering' models that can inform and motivate decisions about interventions.
It is far from clear that public health management was well-served during the critical periods of 2020. A great deal of what was projected to the public was long on data (much of which was, understandably, of mediocre to low quality) and on diagrams and graphs (which were generally of high presentation-quality, but a great many of which appeared to have dubious informational value, driven by availability of data rather than by relevance).
The focus of public health management is "population-based health protection and promotion" (Novick & Morrow 2008, p.60), with efforts "organized and directed to communities rather than to individuals", and with the prevention and control of epidemics high on the priority-list (Novick & Mays 2008, p.3). Key functions and practices are (Novick & Morrow 2008, pp. 40-47):
The target-area for modelling activities to support public health management is accordingly the processes of the spread of the disease, but in such a manner that insights can be delivered to policy-makers regarding the shape that interventions may usefully take, and their likely contribution to containing that spread.
An important distinction is made in decision theory between factors that are strategic or controllable and those that are environmental or uncontrollable (Peterson 2009). A further distinction is necessary between directly-controllable factors and those that can only be indirectly influenced. For example, outputs include published government advice, formal declarations and laws, whereas outcomes comprise the acts of individuals, which are only influenced, not determined, by advice, declarations and laws. The extent to which public behaviour is compliant with the intentions of public health managers depends on controllable factors such as expression, channels of communication and timing, and on factors that are far less controllable, such as attitudes to authority, perceptions of the health threat, and prior experience of government actions.
Even some of the key weapons in the public health arsenal are less directly controllable than might appear to be the case. Health care facilities generally, and aged care facilities in particular, may not be sufficiently reliable in their application of established procedures in relation to hygiene and clinical-grade personal protective equipment. This is especially likely where pressures to reduce costs have been dominating quality factors.
Two of the key weapons in fighting epidemics are quarantine and isolation. The term 'quarantine' applies to people who have been, or are suspected to have been, exposed to an infectious disease, but who are not at that stage known to be infected. Its use in English for this purpose dates to at least the 17th century. The term 'isolation', on the other hand, is applied to people known to be infected. It appears to have been used in this manner since the late 19th century. However, supervision of suspect-quarantine and infectee-isolation may be dependent on inadequately-trained staff, contractors or military personnel. Travel restrictions are difficult to police. Records of attendance at venues are maintained by individuals and venue-operators, and assurance of data quality and data-compatibility is challenging. The implementation of border restrictions may be haphazard where multiple agencies are involved, and particularly so in countries with two or more jurisdictional layers and where borders are a national matter whereas health is a responsibility of subsidiary jurisdictions (states, provinces, departments, Länder, cantons).
Public health activities inherently involve a very broad range of stakeholders, and great diversity among perspectives and values spanning the social, economic and psychological dimensions. As a result, decisions are actively contested, and the decision-making processes complex and at best only modestly well-structured. The Vroom-Yetton-Jago Decision Model identifies five decision-making implementation styles (Vroom & Yetton 1973, Vroom & Jago 1988). For decisions that have significant impact and require input and 'buy-in' from many participants, the relevant two of the five are consultative (group-based but leader-decided) and collaborative (group-based and group-decided).
Because many stakeholders are involved, policy-makers are confronted by diverse views and a rich choice of experts, of approaches to models, of assumptions inherent within them, and hence of the findings presented by the modellers. For consultative and collaborative processes to be effective, participants need to have a shared understanding of the relevant domain and of the terminology used to describe it.
Models can contribute to that understanding by reflecting the key features of real-world systems that policy-makers seek to influence. Further, because pandemics develop in unpredictable ways, and new information and insights become available, policy-makers' appreciation of the context is adaptive. It is therefore crucial that policy-makers develop a degree of clarity about the context in which they are working, communicate that to modellers, and update modellers on changes in their perceptions of the relevant systems.
The most effective way in which modellers can contribute is therefore to start with an appreciation of the relevant domain, to become familiar with the policy-makers' initial mental models, and to be sufficiently 'embedded' to detect changes in their thinking. Further, modellers must convey enough information about their purposes, their assumptions, the capabilities and limitations of their methods, the nature, quality and quantum of the data that they are using, and the extent to which it has and has not been feasible to test findings against the real world. Without great care, there is a high probability of misunderstandings, and of policy-makers being misled.
The following sub-section considers how a particular form of modelling can be used to address these needs.
Multiple forms of modelling exist. At the strategic level, for example, system dynamics is appropriate (Brailsford & Hilton 2000, Brailsford et al. 2014). A particular modelling approach that matches well to the needs of public health management during a pandemic is discrete-event simulation (DES) (Allen et al. 2015). DES modelling involves the identification of the various states that an entity (in this case a person) may be in, their transitions or flows from one state to another, and the factors that determine when transitions occur. A systematic review of publications on DES in health care, in Zhang (2018), concluded that DES has "rich potential ... to provide a broader picture of ... health care systems behavior" (p.9).
Guidance is provided by Sadsad & McDonnell (2014). An example of an application to the treatment of Parkinson's disease is reported in Lebcir et al. (2017). More pertinently, Bai et al. (2018) provide a literature review of the use of DES to model ICU in hospitals. Currie et al. (2020), in discussing the application of simulation modelling technique to the COVID-19 pandemic, describe DES models as being "typically used to model the operation of systems over time, where entities (people, parts, tasks, messages) flow through a number of queues and activities. They are generally suitable for determining the impact of resource availability (doctors; nurses), on waiting times and the number of entities waiting in the queues or going through the system" (p.85). The Currie article identifies a range of potential applications of DES in the context of the pandemic. In Wood et al. (2020), a report is provided of a DES model "designed to capture the key dynamics of the intensive care admissions process for COVID-19 patients" (p.1).
Research has also been published on the application of DES to broader issues than health facility management, such as Bolla & Sarl (2020), who model flows of COVID patients in Switzerland from home to hospital to ICU and beyond and Jalayer et al. (2020), who model "citizens living, working, pursuing their needs and travelling inside a geographical environment" (p.3). Price & Propp (2020, pp.5-14) provide a framework for assessing the suitability of systems dynamics models in informing COVID-19 policymaking, which also has application to DES models.
In Shea et al. (2020), it is suggested that effective use of models depends on combining expert elicitation methods and a structured decision-making framework. Rhodes et al. (2020) perceive models for policy to "blend various heterogeneous data (quantitative, qualitative, abstract, empirical) from various diverse contexts (different viruses, countries, localities, studies, historical periods) ... to enable a decision" (p.2). The authors discuss an "approach to the modelling of pandemics which envisages the model as an intervention of deliberation in situations of evolving uncertainty" (p.1). "The model, precisely because it has latitude as a space of triangulation and speculation, potentiates a working relationship, in which dialogue is made possible" (p.6).
Many researchers assume that DES models have to be fed quantitative data, and that the calculations are what matters. For example, the text elided from the p.2 quotation from Shea et al. (2020) in the previous paragraph is "[blend] into a single calculative process". This ignores the considerable limitations on the usefulness of quantitative analysis in such circumstances, whether conducted mathematically or numerically by experimentation. For example, a comparison across four models of the path of COVID-19 infections in South Africa (Chi et al. 2020) found very wide variation in the models' predictions of case-counts and death-counts, highlighting the folly of reliance on any of them. Similarly, the performance of countries during 2020 was poorly correlated with the results of a 2019 study specifically of preparedness for handling an epidemic (GHS 2019).
The Rhodes et al. article overlooks the fact that the 'blending', the 'deliberation', the 'speculation', the 'working relationship' and the 'dialogue' are all highly valuable in their own right, and may offer far better value to policy-makers than unverified rules applied to mediocre-quality data in a 'calculative process'. Table 2 identifies ways in which a suitable DES model can be applied in the style of a decision support system to enable Vroom-Yetton-Jago consultative or collaborative policy decision-making.
___________________________
To the extent that the model is adequately articulated, tested for logical completeness, and checked against real-world activities, it is also capable of being used to simulate flows of people through the system, and 'stocks' of people currently in each state. This approach would need to be supplemented by a segmentation analysis, distinguishing in particular:
A big-picture view encourages questions to be considered such as:
By manipulating key parameters (such as detection-rate; the proportion of infectees needing admission to hospital and to ICU; hospital- and ICU-capacity; treatment-periods; and mortality-rates), estimates can be made of the limits to the ability of health facilities to cope, and the extent to which urgent investment in additional facilities might be necessary. Hence, in addition to the primary purpose of supporting public health management activities, the model may contribute to the adjacent levels of health facility management and population management, particularly in relation to contact-tracing and social interventions to ensure the effectiveness of quarantine and isolation measures.
The purpose of this research was to investigate the extent to which a DES model could support public health management in the context of a rapidly-developing epidemic. During March-April 2020, I postulated a state-transition model, intended to represent the population of a jurisdiction, and the flow of individual members of it through various states associated with infection, hospitalisation, to recovery or death. The intention was to commence with the minimum complexity, in terms of the number of states, flows, and data about each, based on the available information about the challenges that public policy-makers were addressing. The model could then be experimented with, and expanded to the extent necessary to embody a sufficiently rich understanding of the public policy problem-space. Based on government publications and media reports, and taking account of previous SEIR(D) models, it appeared that the model would need to incorporate about a dozen states, 30-40 flows, and data-items representing the key attributes of the people passing through the system.
Although such a DES model can be applied computationally, that was not the intention, because the complexities and dynamism of the relevant part of the real world are such that the results would inevitably be spurious. The model is intended as a framing tool for the problem-space, intended to help policy-makers formalise their own mental models, appreciate and resolve differences among those models, experiment with the model, and draw inferences relevant to the many decisions they needed to make during the weeks and months of the epidemic.
The first iteration of the model was completed in April 2020. Broadly, individuals were conceived as beginning as Uninfected, with a proportion passing through Infection, possibly via Hospitalisation, and on to Immunity or Death. Each of the four broad domains was conceived as encompassing a number of states, such as being in hospital, or in ICU, or in a queue to get into one of them. Various aspects of each state required some articulation, and so did the conditions under which transitions occur between states. The following section outlines the steps undertaken in order to assess the potential of this model to support public health policy decision-makers.
During the process of postulating the model, a variety of design issues arose. Some were formal questions, such as whether and on what basis some of the state-transitions could logically arise, and could be appropriately represented. For example, it quickly became apparent that the representation of Testing as a state was inappropriate. A more useful approach was to specify attributes of each individual, which travelled with them as they passed through the network. The key attributes appeared to be tested-awaiting-result, tested-negative, and tested-positive. That removed one state and four flows, with no loss of model richness. Many other issues, however, were concerned with the appropriate representation of real-world states and processes. In April 2020, it was too early to resolve those issues, with the result that the initial model was provisional, even tentative.
In order to implement the demonstration phase of Peffers' design science method, experience needed to be gained concerning the relevant real-world systems and the appropriateness or otherwise of the representation of them in the model. A conventional way to gain such experience is through case studies. However, as the COVID-19 pandemic was only just developing, no directly-relevant case studies were available. Although case studies of other pandemics could have been sought out, it was already clear that there were distinct differences between the COVID-19 pandemic and other well-documented events, even other coronavirus events.
A more appropriate method might therefore have been to conduct a contemporaneous field study, seeking embedment within some particular jurisdiction's public health policy apparatus, and preparing a longitudinal case study of that jurisdiction's path, including uncontrolled events, interventions, and subsequent experiences. However, such access would have been very difficult to negotiate, not least in a context in which physical distancing was being imposed. It would also have to a considerable extent limited the testing and articulation process to the factors that arose in a specific jurisdiction. Each country has its own context, conditioned by many cultural factors, and the events, the details of the interventions, the sequences of events, and the timings of events, varied greatly among different jurisdictions. It would be very challenging to try to draw generically useful inferences from such a field study.
An alternative approach was accordingly formulated. Monitoring was undertaken of the ongoing reporting of developments, interventions and experiences in countries worldwide. These reports provided a wide range of circumstances against which the efficacy of the model could be reviewed. This section summarises information about interventions, and identifies and briefly discusses some key themes that emerged.
Governments around the world responded to COVID-19 with a wide range of interventions intended to protect public health. A scan was undertaken of documents published by relevant international and national government agencies, including WHO (2020d) and ICAO (2020), supplemented by academic articles and media reports. Table 3 identifies mainstream public health interventions, clustered into six groups. It is important that IS and IT be brought to bear to assist policy-makers to judge the likely effectiveness of these actions in particular contexts, to design interventions, and to time and manage their implementation, adaptation and eventual withdrawal.
Case Discovery and Management
• Identification of suspects
• Quarantine of suspects
• Management of suspects
• Testing of suspects
• Isolation of infectees
• Contact-tracing of infectees
• Communication with contacts
• Management of contacts
| Facility Restrictions and Closedown
• Hospitals
• Aged care facilities
• Institutions, e.g. prisons
• Group accommodation,
e.g. backpacker dormitories
• Face-to-face businesses
(shops, personal services, gyms)
• Workplaces
• Entertainment venues
• Public gatherings
• Geographical areas (cordon sanitaire)
• Pre-schools and schools • Tertiary educational institutions |
Personal Protection
• Hand hygiene
• Respiratory etiquette
(sneeze/cough protection)
• Avoidance of surfaces
• Face-masks
• Clinical Personal Protective Equipment (PPE) in hospitals and aged-care facilities | Environmental Measures • Cleaning of surfaces |
Physical Distancing Requirements
• Physical distancing in public places
(1.5m / 4sqm)
• Quarantining of suspects
• Isolation of infectees
• Count-limitations on public gatherings
• Curfews on entertainment venues
• 'Work-at-Home'
Recommendations to Employers
• 'Stay-At-Home' Recommendations for at-risk segments | Travel-Related Interventions
• Border restrictions
• Border screening and testing
• Border closure
• Stay-at-home, work-at-home
• Domestic movement restrictions:
• Public transport
• Private vehicles • Walking |
Because the infection-vector appeared to be primarily brief, airborne transmission from infectees to those close by, physical separation among people generally (widely referred to using the misleading term 'social distancing') loomed large among the interventions used. Physical separation is also the objective of quarantine and isolation. Despite the differences in meaning, and the clear explanations provided by a range of national health agencies (e.g. CDC (2020), some agencies were not consistent in their uses of the terms. As a result, media reports evidenced considerable confusion, and it is very likely that many people were unclear about the obligations of suspects, of contacts and of infectees.
Countries around the world adopted vastly different approaches to interventions, recognised different triggering events, and timed their interventions differently. Most also changed their approaches over time. Despite the enormous differences in context, some comparisons are feasible, such as among Scandinavian countries. Sweden implemented only limited actions (physical distancing, bans on large gatherings, and travel restrictions), whereas its neighbours used additional and stronger interventions to reduce the opportunity for the virus to spread, including closedown of many more categories of venue, curfews and border closures. The outcome was a death-rate per capita in Sweden during 2020 that was 4-9 times those of its neighbours (Barrett 2020).
There may also be lessons to be learnt from the juxtaposition of the apparently worst examples of mismanagement and/or outcomes (in particular, the UK, the USA, Belgium, Brazil) and the most successful (e.g. China, Singapore, New Zealand, Australia). The UK flirted with a no-action 'strategy' rationalised as striving for herd immunity, overrode professional advice, lacked coherent and consistent leadership, reacted slowly to new information, and continually changed tack in a haphazard manner (Minghella 2020). A wide range of media reports and some semi-formal reviews gave rise to the list of public health management behaviours associated with serious failure in Table 4.
_____________________
On the other hand, the most successful countries acted quickly and decisively. A range of interventions, and characteristics of interventions, were associated with success in preventing spread and/or reining in spread that had already begun (e.g. OxCGRT 2020). The list of actions in Table 5 was prepared on the basis of reports about actions and outcomes in China (BBC 2020), New Zealand (Baker et al. 2020, Jefferies et al. 2020), Melbourne (Gn 2020a), and Vietnam and Taiwan (Whitworth 2020). See also the analysis of the apparent impacts of testing, contact tracing, and aggressive and early stringency measures, in Pietz et al. (2020).
_____________________
Policy-makers needed to make judgements about which interventions were needed, the specifics of their design and application, and the timing of introduction, easing, and suspension. Their judgements were affected by a great many factors. The efficacy of some actions was apparent from the beginning of the pandemic, whereas the value of other actions emerged slowly, with the gradual accretion of understanding.
In order to balance health safety against social and economic disruption, it was vital to be able to judge the appropriate length of time for quarantine of suspects and isolation of infectees. That depended on the ability to make reasonable determinations about the default period of confinement (requiring an estimate of when infection occurred) and the circumstances under which shorter and longer periods may be appropriate. A guideline for discontinuing transmission-based precautions that was available in mid-2020 was that patients could be released 10 days after symptom onset plus 3-4 days without symptoms, or, in asymptomatic cases, 10 days after a positive test (WHO 2020a). In some countries, that was later variously extended to 14 days, or adjusted to permit discharge as soon as a negative test result was received. This reflected judgements made about the balance between the risk of transmission and the risk of reduced public support and hence compliance levels. In order to support analyses, the model needed to embody additional attributes, such as dates and results of tests for the infection.
An important aspect of the public health problem is advance warning about the capacity of health facilities to cope with demand. It would be a valuable contribution if the model were able to assist in projecting demand for and supply of hospital-beds and ICU beds, in total, and by geographical area and hospital. This may be affected by recent testing rates, positive-result rates, hospitalisation-rates of positive cases, the proportion admitted to ICU, and the periods patients spend in those facilities. The source-data would need to be collected on an ongoing basis, in order to ensure that current indicators were readily to hand. This draws to attention another important attribute of individuals: non-COVID admissions to hospital queues and onwards. Factoring that in enables total demand for hospital and ICU beds to be modelled, and avoids confusing non-COVID-related transitions with those arising from the epidemic.
One of the challenging questions was the extent to which all infectees have much the same degree of infectiveness, or whether there are 'super-spreaders' who are much more prone to infecting other people and/or contaminating surfaces. If there is considerable variability, effort could be valuably invested in determining what infectee-attributes are associated with 'super-spreaders' and whether it is possible to focus available tracing and quarantine resources on people with those attributes. A complication arose to the estimation of infectiveness when, at the end of 2020, strains of the virus emerged that appeared to be substantially more infective.
The importance of the category of people in the state Undetected-Infected became apparent as the epidemic unfolded in each country, because undetected infectees are a primary source of virus-spread, and particularly of very high new-infection rates. In order to gain an insight into the overall progress of the epidemic at a population level, an estimate is needed of the Undetected-Infected status, for example by means of adequate stratified-random-sample testing of the public for the virus. Strategies are needed to find more of the people who are in that state, so that they can be requested or required to shift state to Isolated. Possibilities include extensions to contact-tracing, suspect-definition based on locations and time-periods, infection-testing in the vicinity of hotspots, and random infection-testing. It may be possible to estimate the scale of the count in the Undetected state, by random-testing for antibodies in order to develop estimates of the cumulative count in Undetected-Recovered, and to then reason back from there to the scale of current Undetected-Infecteds. To reflect the uncertainties, there are benefits in using ghostly outlines to represent both Undetected-Infected and Undetected-Recovered, and inflows to those two states. On the other hand, transitions are visible when an individual moves from Undetected to Detected or Hospital-Queue.
Considerable discussion arose about the 'excess mortality' statistic, and the ways in which COVID-19 affected that measure. It became clear that the terminal state Dead needed to be categorised more finely. Cause of death needed to distinguish cases where COVID-19 was the cause of death, or was a significant factor in the death because it compounded prior conditions from all other causes of death, including not only where COVID-19 was not present, but also where infection was, or was assumed to be, present at death but was not listed as a cause.
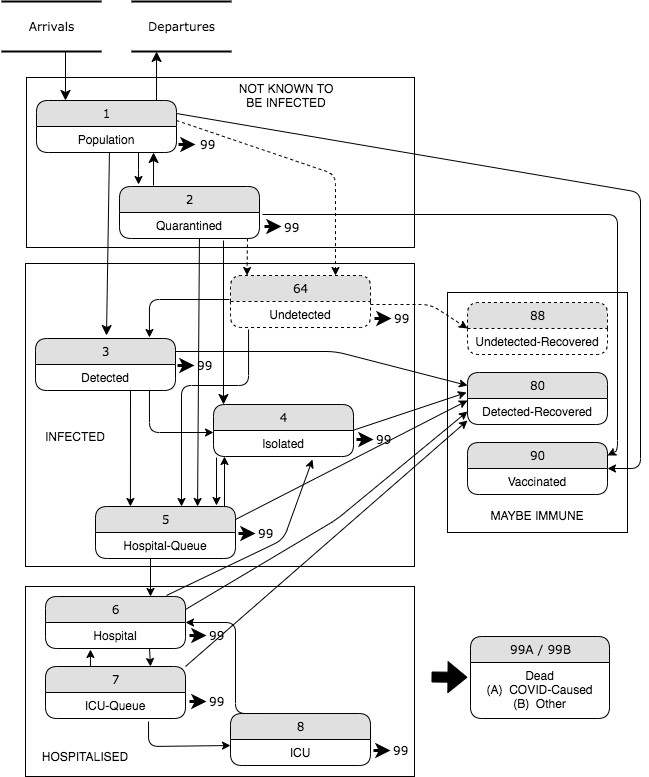
This phase of the research stimulated reconsideration of many aspects of the initial model of April 2020, in order to ensure that it could assist policy-makers in navigating their jurisdiction's particular maze. The result was the revised model in Figure 3, incorporating many adaptations reflecting the insights arising from eight months of vicarious learning from many different jurisdictions. Further detail on the revised model is provided in the underlying Working Paper (Clarke 2021).
Many publications in the IS discipline offer implications for research, but omit discussion of what the work means for practitioners. Research that is intended to be relevant to public policy, on the other hand, needs to focus firstly on implications for practice, with further considerations identified that are addressed to fellow researchers.
The research reported here identifies considerable potential for modelling to provide decision support, not based on computation, but as a tool for individual thought and shared group understanding and discussion. There are challenges, however, in integrating the modelling approach within existing practices. At the end of 2020, each team of policy-makers (of which there were several hundred in national and sub-national jurisdictions throughout the world) was confronted by a second wave of COVID infections and deaths, strained capacity in hospital and ICU facilities, strained relationships with the public, and ongoing financial damage to individuals and harm to national economies. The injection of modellers into the process would cost policy-makers a great deal of time, in order to familiarise the researchers with their methods, to familiarise themselves with the model, and to adapt practices developed during the preceding year of sometimes frantic policy formation and adaptation. This would detract from ongoing, vital activities.
An alternative approach is to seek mind-share by running workshops with policy-makers, adjacent to, rather than embedded within, their actual work. Those currently involved are likely to be currently assigning very low priority to personal training and development. However, individuals who have done a cycle of service during this or a previous pandemic could be appropriate participants. Failing that, proxies for the relevant policy-makers could be considered, such as junior staff or 'understudies' of those currently performing the function, or policy-oriented staff participating in executive development activities, whether within their employment or through postgraduate studies and executive MBA courses.
The work reported in this article suggests that IS research opportunities are being missed. Modelling generally, and DES modelling in particular, appear to be capable of delivering value as a decision support tool in contexts that feature environmental complexity, many stakeholders, and diversity among the stakeholders' value-sets. In addition to public policy areas, many such circumstances arise in business. Other modelling techniques may also be brought to bear. One is system dynamics, at the strategic level. Another is agent-based modelling (ABM), which is applicable where it is important to embody the scope for autonomous entities to take independent action (Hunter et al. 2017, Tracy et al. 2018).
More specifically, further research is needed to assess the usefulness of the particular model depicted in Figure 3. Because the contexts vary enormously across countries, it is important that such an evaluation be conducted in multiple settings, with jurisdictionally and geographically dispersed teams of modellers and policy-makers. The previous section identified the challenges in undertaking an action research approach. It could be feasible to depend on case studies as a basis for once-removed analysis of the model's applicability and usefulness. However, considerable detail is needed, and little of the required information is to be found in media articles, nor in the few more formal reports by academics and government agencies. The alternative of developing a set of case studies for the specific purpose, meanwhile, is scarcely less challenging than the action research approach, because it also requires something close to embedment within the process.
A further implication for researchers relates to the dissemination of research findings in dynamic environments that feature short-half-life informational value, and consequential urgency of publication. A very large number of articles have been published during 2020 in the medical, public health management and social policy literatures. In the IS discipline on the other hand, significant contributions of relevance to public policy have been few and far between. By the end of 2020, the AIS eLibrary disclosed only 3 journal articles addressing COVID-19, and they merely discussed its impacts, variously on digital transformation (in MISQE), on shopping (in PAJAIS), and on research and education (in BISE). See also Thomas et al. (2020) (in BISE, but missing from the AISeL index). That article has relevance to the analysis discussed here, because it includes consideration of how to assist in understanding crises, how to manage health care capacity, and how to help in the implementation of mitigation strategies.
The AIS eLibrary was searched for ICIS'20 papers, because it was held at the end of the first COVID year. No refereed papers with the term in title were found. This appears to be an error, because Ghose et al. (2020) is a Completed Research Paper - although not relevant to the current work. Of the four Short Papers, one (Baier et al. 2020) makes a contribution to analysis of the effectiveness of policy measures.
Every other discipline was generating large volumes of well-considered contributions, but IS was seriously late to the party. However, that is only one of the inadequacies evident in the discipline's performance. Multiple IS conference papers have mentioned the pandemic in passing, but, to the extent that papers have had the topic in focus, they have made little or no contribution to responses by government to the pandemic. It might be natural to expect narrow U.S. MIS venues to be concerned primarily with the impacts of COVID-19 on business, with social responsibility as a constraint rather than social value an objective, as in a Guest Editorial in MISQ Executive in 19, 2 (Watson et al. 2020). However, it is of greater concern that Panels at AMCIS and at ICIS during 2020, and the AIS Forum on the topic, had their focus squarely on impacts of COVID-19 on the IS field and academic community. This inverts Kennedy's exhortation to 'Ask not what we in IS can do for others - ask what environmental factors may do to us in IS'. The AIS's recently-adopted Code of Ethics commences with "1.1 Contribute to society and to human well-being, acknowledging that all people are stakeholders in computing" (AIS 2019). It is not clear that this is being adequately reflected in the Association's activities.
One Basket of 8 venue, the European Journal of IS (EJIS), reflected the fact that the lead-time for research, multi-phase review and queueing for allocation to a journal Issue, is 18 months to 4 years, and hence that COVID-relevant publications would be essentially absent from leading IS journals throughout the likely lifetime of the pandemic. EJIS accordingly announced a 4-Issue series of 'Special Communications' (Agerfalk et al. 2020). This published 13 moderate-length and moderately-refereed articles, during the 2nd to 4th quarters of 2020. The delays from submission to acceptance averaged 2 months (range 0.5 to 4.0), and from submission to publication 4 months (range 1.5 to 7.0). Of these, 6 were relevant to the policy matters under consideration in the present paper (Pietz et al 2020, Trang et al. 2020, Rowe et al. 2020, Sakurai & Chughtai 2020, Adam et al. 2020, Riemer et al. 2020). There are many elements of research quality; but to the extent that IS research purports to have relevance, the delay-factor between completion of research and its communication to the target audience(s) must be drastically reduced. To achieve that outcome, EJIS' 'Special Communications' category needs to be not an exception but a norm, and to be applied by IS journals generally.
Despite great contemporary enthusiasm for IT, it delivered relatively little value during the COVID-19 pandemic of 2020. This appears to have been attributable to an 'applied' approach, 'throwing technology at the problem' and at worst matching the caricature of 'when you have a hammer in your hand, everything looks like a nail'. The tendency has been derided by some commentators as 'technological solutionism' (Morozov 2013).
It appears more likely that IT can deliver for society and the economy if the approach adopted is both more strategic in nature, and 'instrumentalist' / problem-oriented rather than 'applied' / tool-oriented. That means standing far enough back to be able to identify and describe the problem-space, and then modelling the key aspects of that space. Building on that firm foundation, architectures, process models and data models can emerge and be refined, that will much better serve the needs of decision-makers.
The scale of public policy activities during the COVID-19 pandemic, even within each individual jurisdiction, has been so great that a detailed assessment of the models used during 2020 is difficult to assemble. The research reported in this paper comprised a mixture of thought-experiment, abstract design, and testing and adaptation of the initial model against information arising from experience across the world during the period April to December 2020. A model was initially postulated that was envisaged as being suitable as a supporting tool for public policy decisions in relation to public health management. On the basis of new information streaming in during the subsequent months, the need for refinements was apparent. The revised model is capable of further articulation, through specification of data models in support of states and flows, and alternative processing rules for state transitions.
An example of the kind of development that requires rapid adaptation was the mid-January 2021 revelation that the hospital readmission rate in the UK for people who had recovered from COVID-19, during January to September 2020, was 30% - 3.5 times that for the population generally - and that 12% died following discharge - 7 to 8 times that for matched control groups Ayoubkhani et al. 2021). This suggests that the incidence of 'Long COVID' or 'Post-COVID Syndrome' (PCS) may be much higher than previously thought. It also raises questions about the extent to which people in the Recovered and even Vaccinated states are immune to COVID-19, and even whether they are incapable of becoming infective again.
The work reported here opens up a variety of possibilities for further research, including:
The model proposed and tested in this paper has, by its nature, limited focus. Its target-area is expressly public health management, although it has application also to the adjacent level of health facility management, and implications for population management. It is not suggested that this model subsumes or replaces models at other levels of abstraction. It is contended, however, that public health policy-makers, and government ministers and their advisers, can greatly benefit from the development, articulation and ongoing adaptation of a model of this nature. It enables processes to be better understood, strategies considered, and implications of possible interventions thought through. This information can then be combined with that arising from work at other levels of abstraction (bio-medical and medical, on the one hand, and public behaviour management and economic management on the other).
The project reported on in this article provides an example of an IS research making contribution to an important public policy matter. The work applied a well-established modelling technique, but not in a manner that emphasises decision-making, nor even quantitative input to decision-makers. In the complex, uncertain, multi-dimensional and value-laden contexts that are common in the public policy field, the emphasis is on process aspects of decision support, assisting policy-makers with diverse perspectives to work towards a common mental model of the problem-space, and a shared understanding of the specialist dialect in use. This research accordingly also represents a contribution towards the maturation of the IS discipline in the area of public policy, through support for the conception, shaping and evaluation of interventions.
Adam M., Werner D., Wendt C. & Benlian A. (2020) 'Containing COVID-19 through physical distancing: the impact of real-time crowding information' European Journal of Information Systems 29, 5 (Sep-Oct 2020) 595-607, at https://orsociety.tandfonline.com/doi/full/10.1080/0960085X.2020.1814681#.YCi6jC1L1oM
AG (2020) 'Privacy-Preserving Contact Tracing' Apple and Google, April-September 2020, at https://covid19.apple.com/contacttracing
Agerfalk P., Conboy K. & Myers M. (2020) 'Call for Papers: Special Communications on Information Systems in the Age of Pandemics' The European Journal of Information Systems, undated but apparently of May/June 2020, at https://www.journalconferencejob.com/ejis-is-pandemics
AIS (2019) 'AIS Code of Ethics and Professional Conduct' Assocxiation for Information Systems, 14 December 2019, at https://aisnet.org/general/custom.asp?page=MemberCodeOfConduct
ALI (2021) 'International monitor: vaccine passports and COVID status apps' Ada Lovelace Institute, February 2021, at https://www.adalovelaceinstitute.org/project/international-monitor-vaccine-passports-covid-status-apps/
Allen M., Spencer A., Gibson A., Matthews J., Allwood A., Prosser S. & Pitt M. (2015) 'What is discrete event simulation, and why use it?' Chapter 5 of 'Right cot, right place, right time: improving the design and organisation of neonatal care networks - a computer simulation study' NIHR Journals Library, May 2015, at https://www.ncbi.nlm.nih.gov/books/NBK293948/
Aron J.L. & Schwartz I.B. (1984) 'Seasonality and period-doubling bifurcations in an epidemic model' J. Theor. Biol. 110:665-679, 1984, at https://www.researchgate.net/profile/Ira_Schwartz/publication/16673793_Seasonality_and_period-doubling_bifurcations_in_an_epidemic_model/links/59d7a186a6fdcc2aad0645fc/Seasonality-and-period-doubling-bifurcations-in-an-epidemic-model.pdf
Ayoubkhani D., Khunti K., Nafilyan V., Maddox T., Humberstone B., Diamond I. & Banerjee A. (2021) 'Epidemiology of post-COVID syndrome following hospitalisation with coronavirus: a retrospective cohort study' medRxiv, 15 January 2021, at https://www.medrxiv.org/content/10.1101/2021.01.15.21249885v1
Bai J., Fu_gener A., Schoenfelder J. & Brunner J.O. (2018) 'Operations research in intensive care unit management: a literature review' Health Care Manag Sci (2018) 21:1-24 DOI 10.1007/s10729-016-9375-1
Baier L., Schoeffer J. & Ku_hl N. (2020) 'Utilizing Adaptive AI-based Information Systems to Analyze the Effectiveness of Policy Measures in the Fight of COVID-19' Proc. ICIS 2020, 4, at https://aisel.aisnet.org/icis2020/is_health/is_health/4
Baker M.G., Kvalsvig A. & Verrall A.J. (2020) 'New Zealand's COVID_19 elimination strategy' Med J Aust 213, 5 (September 2020) 198-200, at https://www.mja.com.au/journal/2020/213/5/new-zealands-covid-19-elimination-strategy
Barrett M. (2020) 'What have Norway, Finland and Denmark got right on Covid-19?' New Statesman, 22 December 2020, at https://www.newstatesman.com/world/europe/2020/12/what-have-norway-finland-and-denmark-got-right-covid-19
Baskerville R., Pries-Heje J. & Venable J. (2009) 'Soft Design Science Methodology' Proc. 4th Int'l Conf. on Design Science Research in Information Systems and Technology (DESRIST 2009), Philadelphia PA, at https://dl.acm.org/doi/pdf/10.1145/1555619.1555631?casa_token=zErR3NVLlv4AAAAA:ILFAZnLN0OBuSK0UU2LUZIkNXDegAiaKZDO46Hmw9aqWPC-22nBZQocBqXmwv--uqO1QGwt2zpx1nA
BBC (2020) 'Covid-19: China's Qingdao to test nine million in five days' BBC News, 12 October 2020, at https://www.bbc.com/news/world-asia-54504785
von Bertalanffy L. (1968) 'General System Theory: Foundations, Development, Applications' George Braziller, 1968
Bilandzic M. & Venable J. (2011) 'Towards Participatory Action Design Research: Adapting Action Research and Design Science Research Methods for Urban Informatics' Journal of Community Informatics 7, 3 (2011), at https://espace.curtin.edu.au/bitstream/handle/20.500.11937/49022/248627.pdf?sequence=3
Bolla P. & Sarl A. (2020) 'Using Discrete Event Simulation model to simulate COVID19 epidemics in Switzerland' ALASS, August 2020, at 20/2/21 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7341703/
Brailsford S., Churilov L. & Dangerfield B. (eds.) (2014) 'Discrete_Event Simulation and System Dynamics for Management Decision Making' Wiley, 2014
Brailsford S. & Hilton NB. (2000) 'A Comparison of Discrete Event Simulation and System Dynamics for Modelling Healthcare Systems' Proc. ORAHS 2000, Glasgow, pp. 18-39, at https://eprints.soton.ac.uk/35689/1/glasgow_paper.pdf
Braithwaite I., Callender T., Bullock M. & Aldridge R.W. (2020) 'Automated and partly automated contact tracing: a systematic review to inform the control of COVID-19' The Lancet Digital Health 2, 11 (November 2020) e607-e621, at https://www.sciencedirect.com/science/article/pii/S2589750020301849
Brauer F. (2008) 'Compartmental Models in Epidemiology' Springer, Lecture Notes in Mathematics, volume 1945, pp. 19-79, at https://link.springer.com/content/pdf/10.1007%2F978-3-540-78911-6_2.pdf
vom Brocke J., Watson R.T., Dwyer C., Elliot S. & Melville N. (2013) 'Green Information Systems: Directives for the IS Discipline' Communications of the Association for Information Systems 33, 30 (December 2013) 509-520
Budd J., Miller B.S., Manning E.M., et al. (2020) 'Digital technologies in the public-health response to COVID-19' Nature Medicine 26 (August 2020) 1183-1192, at https://www.nature.com/articles/s41591-020-1011-4
CDC (2020) 'Legal Authorities for Isolation and Quarantine' Center for Disease Control, Washington DC, rev. February 2020, at https://www.cdc.gov/quarantine/aboutlawsregulationsquarantineisolation.html
Chi Y.-L., Chalkidou K. & Walker D. (2020) 'What Can Policymakers Learn about COVID-19 from Looking at Different Model Estimates?' Center for Global Development, June 2020, at https://www.cgdev.org/blog/what-can-policymakers-learn-about-covid-19-looking-different-model-estimates
Clarke R. (2020a) 'The Effectiveness of Bluetooth Proximity Apps in Tracing People with COVID-19 Exposure Risk' Xamax Consultancy Pty Ltd, April 2020, at http://rogerclarke.com/EC/EBPA.html
Clarke R. (2020b) 'We need to examine the many narratives of the COVIDsafe app' UNSW Newsroom, 4 May 2020, at https://newsroom.unsw.edu.au/news/business-law/we-need-examine-many-narratives-covidsafe-app
Clarke R. (2021) 'Simulation Modelling for Public Health Management during the COVID-19 Pandemic' Xamax Consultancy Pty Ltd, January 2021, at at http://rogerclarke.com/EC/CVMB.html
Clarke R. & Davison R.M. (2020a) 'Through Whose Eyes? The Critical Concept of Researcher Perspective' J. Assoc. Infor. Syst. 21, 2 (March-April 2020) 483-501, PrePrint at http://www.anu.edu.au/people/Roger.Clarke/SOS/RP.html
Clarke R., Davison R.M. & Jia W. (2020b) 'Researcher Perspective in the IS Discipline: An Empirical Study of Articles in the Basket of 8 Journals' Information Technology & People 33, 6 (October 2020) 1515-1541, PrePrint at http://www.rogerclarke.com/SOS/RPBo8.html
Currie C.S.M., Fowler J.W., Kotiadis K., Monks T., Onggo B.S., Robertson D.A. & Tako A.A. (2020) 'How simulation modelling can help reduce the impact of COVID-19' Journal of Simulation 14:2 (2020) 83-97, DOI: 10.1080/17477778.2020.1751570
Dedrick J. (2010) 'Green IS: Concepts and Issues for Information Systems Research' Communications of the Association for Information Systems 27 (January 2010) 1, at https://www.researchgate.net/profile/Jason_Dedrick/publication/262376624_Green_IS_Concepts_and_Issues_for_Information_Systems_Research/links/56670fca08ae34c89a0224dc/Green-IS-Concepts-and-Issues-for-Information-Systems-Research.pdf
Econ (2020) 'Tracking the coronavirus across Europe' The Economist, 3 July 2020, at https://www.economist.com/graphic-detail/2020/07/03/tracking-the-coronavirus-across-europe
Gault F.D., Hamilton K.E., Hoffman R.B. & McInnis B.C. (1987) 'The design approach to socio-economic modelling' Futures 19, 1 (February 1987) 3-25, at https://www.peakoil.net/files/THE_DESIGN_APPROACH_TO_SOCIO_ECONOMIC_MODELLING.pdf
de la Garza A. (2020) 'Contact Tracing Apps Were Big Tech's Best Idea for Fighting COVID-19. Why Haven't They Helped?' Time Magazine, 10 November 2020, at https://time.com/5905772/covid-19-contact-tracing-apps/
Ghose A., Li B., Meghanath M.Y., Sun C., Foutz N.Z. & Anton J. (2020) 'Trading Privacy for Social Good: Did America Unite During COVID-19?' Proc. ICIS 2020, 13
GHS (2019) 'Global Health Security Index' GHS Index, October 2019, at https://www.ghsindex.org
Giordano G., Blanchini F., Bruno R., Colaneri P., Di Filippo A., Di Matteo A. & Colaneri M. (2020) 'Modelling the COVID-19 epidemic and implementation of population-wide interventions in Italy' Nature Medicine 26 (April 2020) 855-860, at https://www.nature.com/articles/s41591-020-0883-7
Gn (2020a) 'Melbourne Covid lockdown rules and coronavirus restrictions explained' The Guardian, 9 November 2020, at https://www.theguardian.com/australia-news/2020/nov/09/melbourne-restrictions-victoria-lockdown-rules-covid-19-metropolitan-metro-explained-what-you-need-to-know
Gn (2020b) 'Our key findings about US healthcare worker deaths to date' The Guardian, 23 Dec 2020, at https://www.theguardian.com/us-news/ng-interactive/2020/dec/22/lost-on-the-frontline-our-findings-to-date
Greenleaf G. (2020) 'Australia: A poor model for QR data `attendance tracking' Digital Asia Hub, December 2020, at https://www.digitalasiahub.org/2021/01/06/australia-a-poor-model-for-qr-data-attendance-tracking/
Greenleaf. G & Kemp K. (2020) 'Australia's 'COVIDSafe' law for a voluntary contact tracing app' Privacy Laws & Business International Report 165 1 (May 2020) 3-6, at https://ssrn.com/abstract=3589317
Gregor S. & Hevner A. (2013) 'Positioning Design Science Research for Maximum Impact' MIS Quarterly 37, 2 (June 2013 ) 337-355, at https://ai.arizona.edu/sites/ai/files/MIS611D/gregor-2013-positioning-presenting-design-science-research.pdf
Gumel A.B., McCluskey C.C. & Watmough J. (2006) 'An SVEIR Model for Assessing Potential Impact of an Imperfect Anti-SARS Vaccine' Mathematical Biosciences And Engineering 3, 3 (July 2006) 485-512
Hunter E., MacNamee B. & Kelleher J. (2017) 'A Taxonomy for Agent-Based Models in Human Infectious Disease Epidemiology' Journal of Artificial Societies and Social Simulation 20, 3 (2017) 2, at http://jasss.soc.surrey.ac.uk/20/3/2.html
ICAO (2020) 'Public Health Risk Mitigation Measures' International Civil Aviation Organisation, 2020, at https://www.icao.int/covid/cart/Pages/Public-Health-Risk-Mitigation-Measures.aspx
Jalayer M., Orsenigo C. & Vercellis C. (2020) 'CoV-ABM: A stochastic discrete-event agent-based framework to simulate spatiotemporal dynamics of COVID-19' arXiv (Jul 2020), at 20/2/21 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7341703/
Jayadevan R. (2020) 'The 6 most successful anti-Covid strategies so far, and the reasons why they worked' Onmanorama, 3 June 2020, at https://www.onmanorama.com/lifestyle/health/2020/06/03/most-successful-anti-covid-strategies-reasons-why-they-worked.html
Jefferies S., French N., Gilkison C., Graham G., Hope V., Marshall J., McElnay C., McNeill A., Muellner P., Paine S., Prasad N., Scott J., Sherwood J., Yang L. & Priest P. (2020) 'COVID-19 in New Zealand and the impact of the national response: a descriptive epidemiological study' Lancet Public Health 5 (October 2020) e612-23, at https://www.thelancet.com/action/showPdf?pii=S2468-2667%2820%2930225-5
Kermack W.O. & McKendrick A.G. (1927) 'A Contribution to the Mathematical Theory of Epidemics' Proc. Roy. Soc. Lond. A 115, 700-721, 1927, at http://www.math.utah.edu/~bkohler/Journalclub/kermack1927.pdf
Kling R. (1978) 'Automated Information Systems as Social Resources In Policy Making' Proc. Association for Computing Machinery, 1978, pp.666-674, at https://dl.acm.org/doi/pdf/10.1145/800178.810109?casa_token=CZb-QzFZpqkAAAAA:4INvFlBZXt5MZ0zcMfba7YihXplIRDcpvj-dtTFho_Mjtb56STdNNFVs_CjCh8cmDnOiDGTqHmVkNw
Knill C. & Tosun J. (2020) 'Public Policy: A New Introduction' Macmillan, 2nd ed., 2020
Lebcir R., Demir E., Ahmad R., Vasilakis C. & Southern D. (2017) 'A discrete event simulation model to evaluate the use of community services in the treatment of patients with Parkinson's disease in the United Kingdom' BMC Health Services Research volume 17, Article number: 50 (2017), at https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-017-1994-9
Loughran J. (2021) 'Vaccine passports present data privacy risk, MPs warned' Engineerijng & Technology, 26 January 2021, at https://eandt.theiet.org/content/articles/2021/01/vaccine-passports-present-data-privacy-risk-mps-warned/
Minghella D. (2020) 'The UK and Covid-19: the tragedy of the road not taken' New Statesman, 22 December 2020, at https://www.newstatesman.com/politics/uk/2020/12/uk-and-covid-19-tragedy-road-not-taken
Morozov E. (2013) 'To Save Everything, Click Here: The Folly of Technological Solutionism' Public Affairs, 2013
Moss R., Wood J., Brown D., Shearer F., Black A.J., Cheng A.C., McCaw J.M. & McVernon J. (2020) 'Modelling the impact of COVID-19 in Australia to inform transmission reducing measures and health system preparedness' medRxiv, 11 April 220, at http://dx.doi.org/10.1101/2020.04.07.20056184
Mussared J. & Teague V. (2020) 'COVIDSafe issues found by the tech community' Github, July 2020, at https://github.com/vteague/contactTracing/blob/master/blog/2020-07-07IssueSummary.md
Niederman F., Clarke R., Applegate L., King J.L., Beck R. & Majchrzak A. (2017) 'IS Research and Policy: Notes From the 2015 ICIS Senior Scholar's Forum' Communications of the Association for Information Systems 40 (February 2017) 5
Niederman F. & March S. (2012) 'Design Science and the Accumulation of Knowledge in the Information Systems Discipline' ACM Transactions on MIS 3, 1 (2012), 1
Nikulin I.I., Woolverton K.E. & Withington M.J. (2020) 'Using Dynamic Models and Empirical COVID-19 Data to Showcase Effective Pandemic Prevention Measures' Worcester Polytechnic Institute, at https://digitalcommons.wpi.edu/iqp-all/5759
Novick L.F. & Mays G.P. (eds.) (2008) 'Public Health Administration: Principles for Population-based Management' Jones & Bartlett, 2008
Novick L.F. & Morrow C.B. (2008) 'A Framework for Public Health Administration and Practice' Ch. 2 in Novick & Mays (2008), pp. 35-68
ONS (2021) 'Deaths registered weekly in England and Wales, provisional: week ending 1 January 2021' Office of National Statistics, UK, January 2021, at https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsregisteredweeklyinenglandandwalesprovisional/weekending1january2021
OxCGRT (2020) 'Codebook' Oxford Covid-19 Government Response Tracker, v.2.6, 09 December 2020, at https://github.com/OxCGRT/covid-policy-tracker/blob/master/documentation/codebook.md
Peffers K., Tuunanen T., Rothenberger M. & Chatterjee S. (2007) 'A design science research methodology for information systems research' Journal of Management Information Systems, 24, 3 (Winter 2007) 45-77
Peterson M. (2009) 'An Introduction to Decision Theory' Cambridge University Press, 2009
Pietz J., McCoy S. & Wilck J.H. (2020) 'Chasing John Snow: data analytics in the COVID-19 era' European Journal of Information Systems 29, 4 (Jul-Aug 2020) 388-404, at https://orsociety.tandfonline.com/doi/full/10.1080/0960085X.2020.1793698#.YCi73y1L1oM
Price C.C. & Propp A.M. (2020) 'A Framework for Assessing Models of the COVID-19 Pandemic to Inform Policymaking in Virginia' Rand Corp., 2020, at https://www.rand.org/pubs/research_reports/RRA323-1.html
Rhodes T., Lancaster K., Lees S. & Parker M. (2020) 'Modelling the pandemic: attuning models to their contexts' BMJ Global Health (June 2020), doi:10.1136/ bmjgh-2020-002914, at https://gh.bmj.com/content/bmjgh/5/6/e002914.full.pdf
Riemer K., Ciriello R., Peter S. & Schlagwein D. (2020) 'Digital contact-tracing adoption in the COVID-19 pandemic: IT governance for collective action at the societal level' European Journal of Information Systems 29, 6 (Nov-Dec 2020) 731-745, at https://orsociety.tandfonline.com/doi/full/10.1080/0960085X.2020.1819898#.YCi3Xy1L1oM
Rowe F., Ngwenyama O. & Richet J.-L. (2020) 'Contact-tracing apps and alienation in the age of COVID-19' European Journal of Information Systems 29, 5 (Sep-Oct 2020) 545-562, at https://orsociety.tandfonline.com/doi/pdf/10.1080/0960085X.2020.1803155
Sadsad R. & McDonnell G. (2014) 'Multiscale modelling for public health management: A practical guide' Ch. 13 in Brailsford et al. (2014)
Sakurai M. & Chughtai H. (2020) 'Resilience against crises: COVID-19 and lessons from natural disasters' European Journal of Information Systems 29, 5 (Sep-Oct 2020) 585-594, at https://orsociety.tandfonline.com/doi/full/10.1080/0960085X.2020.1814171#.YCi52y1L1oM
Schipper H. (2020) 'How pandemic modelling failed policy-makers, and how to do better' Macdonald-Laurier Institute, July 2020, at https://macdonaldlaurier.ca/files/pdf/July_Commentary_Schipper_FWeb.pdf
Sein M.K., Henfridsson O., Purao S., Rossi M. & Lindgren R. (2011) 'Action Design Research' MIS Quarterly 35, 1 (March 2011) 37-56, at https://www.diva-portal.org/smash/get/diva2:871353/FULLTEXT01.pdf
Shea K., Runge M.C., Pannell D., Probert W.J.M., Li S.-M., Tildesley M. & Ferrari M. (2020) 'Harnessing multiple models for outbreak management' Science 368, 6491 (8 May 2020)
Siebers P.O., Macal C.M., Garnett J., Buxton D. & Pidd M. (2010) 'Discrete-Event Simulation is Dead, Long Live Agent-Based Simulation!' Journal of Simulation 4, 3 (2010) 204-210, at https://link.springer.com/content/pdf/10.1057/jos.2010.14.pdf
Silva C.L.S, Batista P.V.C., Lima H.S., Alves M.A., Guimar<es F.G. & Silva R.C.P. (2020) 'COVID-ABS: An agent-based model of COVID-19 epidemic to simulate health and economic effects of social distancing interventions' Chaos, Solitons & Fractals 139 (October 2020) 110088, at https://doi.org/10.1016/j.chaos.2020.110088
Sprague R.H. (1980) 'A Framework for the Development of Decision Support Systems' MIS Qtly 4, 4 (December 1980) 1-26
SWPRS (2020) 'Post-Acute Covid ('Long Covid')' Swiss Policy Research, August 2020, at https://swprs.org/post-acute-covid-long-covid/
Thomas O., Hagen S., Frank U., Recker J., Wessel L., Kammler F., Zarvic N. & Timm I. (2020) 'Global Crises and the Role of BISE' Business & Information Systems Engineering 62, 4 (June 2020) 385-396, at https://link.springer.com/article/10.1007/s12599-020-00657-w
Tracy M., Cerda M. & Keyes K.M. (2018) 'Agent-Based Modeling in Public Health: Current Applications and Future Directions' Ann. Rev. Public Health 39 (2018) 77-94, at https://www.annualreviews.org/doi/10.1146/annurev-publhealth-040617-014317
Trang S., Trenz M., Weiger W.H., Tarafdar M. & Cheung C.M.K. (2020) 'One app to trace them all? Examining app specifications for mass acceptance of contact-tracing apps' Euro. J. of Infor. Syst. 29, 4 (Jun 2020) 415-428, at https://orsociety.tandfonline.com/doi/full/10.1080/0960085X.2020.1784046
Vroom V.H. & Jago A.G. (1988) 'The New Leadership: Managing participation in organizations' Prentice Hall, 1988
Vroom V.H. & Yetton P.W. (1973) 'Leadership and Decision Making' University of Pittsburgh Press, 1973
Watson R.T. (ed.) (2008) 'Green IS: Building Sustainable Business Practices' University of Georgia, 2008, at https://www.researchgate.net/profile/Richard_Watson5/publication/242112741_Green_IS_Building_Sustainable_Business_Practices/links/0c96053020a8f60253000000/Green-IS-Building-Sustainable-Business-Practices.pdf
Watson R., Ives B. & Piccoli G. (2020) 'Guest Editorial: Practice-Oriented Research Contributions in the Covid-19 Forged New Normal' MIS Quarterly Executive 19, 2 (2020) 2
Weitz J.S. & Dushoff J. (2015) 'Modeling Post-death Transmission of Ebola: Challenges for Inference and Opportunities for Control' Sci Rep 5, 8751 (March 2015), at https://www.nature.com/articles/srep08751
Whitworth J. (2020) 'Lessons from around the world on fighting COVID's second wave' The Conversation, 21 November 2020, at https://theconversation.com/lessons-from-around-the-world-on-fighting-covids-second-wave-150432
WHO (2020a) 'Criteria for releasing COVID-19 patients from isolation: Scientific Brief' 17 June 2020, at https://www.who.int/news-room/commentaries/detail/criteria-for-releasing-covid-19-patients-from-isolation
WHO (2020b) 'Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations' World Health Organisation, Scientific brief, 29 March 2020, updated 9 July 2020, at https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations
WHO (2020c) ' Transmission of SARS-CoV-2: implications for infection prevention precautions: Scientific Brief' World Health Organisation, Interim guidance, July 2020, at https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions#:~:text=The%20incubation%20period%20of%20COVID,to%20a%20confirmed%20case.
WHO (2020d) 'Considerations in adjusting public health and social measures in the context of COVID-19' World Health Organisation, Interim guidance, April 2020, rev. November 2020, at https://www.who.int/publications/i/item/considerations-in-adjusting-public-health-and-social-measures-in-the-context-of-covid-19-interim-guidance
WOM (2020) 'Reported Cases and Deaths by Country, Territory, or Conveyance' Worldometer, December 2020, at https://www.worldometers.info/coronavirus/#countries
Wood R.M., McWilliams C.J., Thomas M.J., Bourdeaux C.P. & Vasilakis C. (2020) 'COVID-19 scenario modelling for the mitigation of capacity-dependent deaths in intensive care' Health Care Manag Sci. 2020 8 (Jul 2020) 1-10, doi: 10.1007/s10729-020-09511-7, at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7341703/
Zhang X. (2018) 'Application of discrete event simulation in health care: a systematic review' BMC Health Services Research volume 18, Article number: 687 (2018), at https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-018-3456-4
An earlier version of parts of this article was submitted to the Bled eConference. Feedback from colleagues was greatly appreciated, in particular from Profs. Dubravka Cecez-Kecmanovic, Graham Greenleaf, Jürgen Seitz, Robin Stanton, Doug Vogel and Nilmini Wickramasinghe.
Roger Clarke is Principal of Xamax Consultancy Pty Ltd, Canberra. He is also a Visiting Professor associated with the Allens Hub for Technology, Law and Innovation in UNSW Law., and a Visiting Professor in the Research School of Computer Science at the Australian National University.
| Personalia |
Photographs Presentations Videos |
Access Statistics |
 |
The content and infrastructure for these community service pages are provided by Roger Clarke through his consultancy company, Xamax. From the site's beginnings in August 1994 until February 2009, the infrastructure was provided by the Australian National University. During that time, the site accumulated close to 30 million hits. It passed 65 million in early 2021. Sponsored by the Gallery, Bunhybee Grasslands, the extended Clarke Family, Knights of the Spatchcock and their drummer |
Xamax Consultancy Pty Ltd ACN: 002 360 456 78 Sidaway St, Chapman ACT 2611 AUSTRALIA Tel: +61 2 6288 6916 |
Created: 5 December 2020 - Last Amended: 20 February 2021 by Roger Clarke - Site Last Verified: 15 February 2009
This document is at www.rogerclarke.com/EC/CVMJ.html
Mail to Webmaster - © Xamax Consultancy Pty Ltd, 1995-2022 - Privacy Policy